The Centers for Medicare & Medicaid Services (CMS) made significant changes to reimbursement rules and rates for medical services in 2021 that will likely impact workers compensation (WC) fee schedules, with some already in effect. This article describes the changes that are most pertinent to the industry and their potential impact on medical costs.
INTRODUCTION
Most states have medical fee schedules that establish maximum allowable reimbursements (MARs) for payments of medical services in WC. Fee schedules vary across states in many ways, from the services they address, to the MARs for those services, and even to the methodologies for setting those MARs. States often rely to some degree on rules and payment rates the CMS publishes and will annually update their fee schedules to reflect the CMS changes.
The CMS published its 2021 final physician fee schedule (PFS) on December 2, 2020, which included notable changes that may significantly impact many states’ WC fee schedules. Then, in response to the “Consolidated Appropriations Act, 2021,” the CMS published an update to the PFS on December 27, 2020.
This article discusses these modifications:
- CMS physician fee schedule changes
- Significant increases to payment rates for evaluation and management (E/M) services
- Expanded services approved to be delivered via telemedicine
- CMS facility fee schedule changes
- Expanded treatments allowed in an outpatient setting by removing procedures from the inpatient-only procedures list
- Increased ambulatory surgical center (ASC) flexibility to offer inpatient services
PHYSICIAN FEE SCHEDULE CHANGES
Evaluation and Management
Payments for E/M services represent about 25% of countrywide1 physician costs in WC. The figure below shows the share of E/M services by state for services provided in 2019.
The 2021 CMS PFS has changes that directly impact E/M services and may indirectly affect other physician services. To understand these impacts, it is important to understand how the CMS sets individual payment rates and how changes to individual payment rates can impact reimbursements for other unrelated services.
Below on the left is the standard formula the CMS uses to calculate the payment rates for individual physician services. On the right is a simplified version, which combines the Relative Value Unit (RVU) terms and excludes the components involving Geographical Practice Cost Indices (GPCIs). The simplified version is helpful to illustrate the potential impacts of the PFS changes.
RVUs vary by service and may also differ depending on whether the service takes place in a facility or practitioner’s office. The conversion factor does not vary by service. The final 2021 CMS PFS includes increases to the RVUs for E/M services. The table below displays a year-over-year comparison of the CMS’s national practitioner’s office RVUs for the most commonly provided E/M services. These services account for more than 75% of the total WC E/M transactions countrywide.
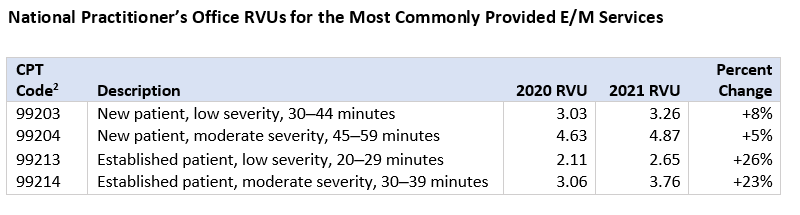
The CMS included these RVU increases to “recognize shifts in medical practice and appropriately reflect resources involved in providing these services, particularly primary care, to manage chronic disease.”3 All else equal, a significant increase to E/M RVUs would cause a notable increase in E/M payment rates and a potential increase in overall Medicare spending. The CMS initially mitigated the impact on total Medicare spending of increases in individual RVUs through a ‒10.2% offsetting adjustment to the 2021 conversion factor. However, based on modifications in the “Consolidated Appropriations Act, 2021,” the CMS published an update to the 2021 conversion factor resulting in a smaller impact equal to ‒3.3%.
The impact on WC medical costs due to the changes in the E/M RVUs and the conversion factor will vary across states—depending on how each state’s WC fee schedule interacts with the CMS PFS and recognizing the effect of any state-specific regulatory action that has occurred. Although there are many variations to how states determine MARs, we will generalize these methodologies for this discussion into three categories based on each state’s reliance on the maximum rates the CMS publishes. Note that states without physician fee schedules are not included in the below categories.
The CMS changes will not directly impact state-specific fee schedules. However, to the extent that such fee schedules depend on factors the CMS changes impact (e.g., neighboring state MARs), an impact could occur to those states’ fee schedules as well.
When states update their Medicare-based or partially Medicare-based fee schedules, they incorporate the most recent CMS changes. Most of these states update their WC fee schedule annually, though some have less frequent updates.
States with partially Medicare-based fee schedules may see significant impacts. In most instances, the state may utilize the higher RVUs the CMS provides and apply its state-specific conversion factors to calculate the final MAR. Even if the state-specific conversion factors remain unchanged, the state’s system costs could potentially increase due to the change in the E/M RVUs.
Estimated impacts due to the increased E/M RVUs range from +1% to +2% on total medical costs in the states with partially Medicare-based fee schedules.
For states with Medicare-based fee schedules, the 3.3% reduction to the conversion factor would impact MARs for all services. This would slightly temper the increase in E/M MARs and would put downward pressure on MARs in all other cost categories. States with Medicare-based fee schedules should still expect medical cost increases, but they will likely be less significant than those possibly expected in states with partially Medicare-based fee schedules.
In addition to increasing RVUs and the corresponding conversion factor decrease, the CMS has adopted the following changes to E/M services:
- Simplified code level selection
- Deletion of level 1 new patient code
The extent of these changes may vary as individual state regulations require different rules for documentation.
For additional information, please see NCCI’s 2019 review of the CMS proposed changes to E/M services in “Evaluation and Management Costs in Workers Compensation.”
Telemedicine
The CMS expanded its lists of telehealth services due to the unprecedented growth in telemedicine as a result of the COVID-19 pandemic. The CMS has permanently added some codes to the telehealth services list, while others are temporary additions.
Permanent additions of services to the CMS’s telehealth list relevant to WC include:
- Group Psychotherapy―CPT code 90853
- Psychological and Neuropsychological Testing―CPT code 96121
Any long-term impacts from these changes are unclear at this time. NCCI will continue to monitor changes in telemedicine usage and how the utilization of telemedicine may impact the delivery of WC medical services.
Additional information on COVID-19 and telehealth services may be found in NCCI’s article “Telemedicine—Covid-19 Affects Medical Service Delivery in 2020.”
FACILITY FEE SCHEDULE CHANGES
Facility costs account for about 40% of WC medical expenditures and were a significant cost driver in recent years. The CMS implemented several amendments that are likely to impact the utilization of different types of facilities and their corresponding costs in WC. The CMS carried out these changes to increase choices and options while seeking to reduce overall costs.
Elimination of the Inpatient-Only List
The inpatient-only list comprises procedures which Medicare would only reimburse when performed in a hospital inpatient setting. The CMS will eliminate the inpatient-only list during a three-year transitional period ending in Calendar Year (CY) 2024.4 Of the approximately 1,700 procedures on the inpatient-only list, the CMS removed about 300 musculoskeletal-related procedures in CY 2021.
Of the musculoskeletal procedures removed from the inpatient-only list in CY 2021, the most commonly performed WC procedure in Service Year 2019 was CPT code 22558 (lumbar spinal fusion), which is a procedure commonly performed on workers diagnosed with lumbar spinal degeneration. Ultimate cost impacts and extents will depend on several factors, including:
- Whether the procedures can be performed safely in an outpatient setting
- Current state experience for the impacted procedures
- The availability of alternative places of service (e.g., ASCs and hospital outpatient surgery centers)
- Surgeon, patient, and insurer behavioral changes
Ambulatory Surgical Center Flexibility
To assist hospitals with stressed capacity from COVID-19 patients, the CMS has outlined a strategy for enabling ASCs to perform procedures commonly conducted in a hospital inpatient setting.
Under these provisions, some ASCs can temporarily register for the CMS to certify them as hospitals. These ASCs could then perform services on patients who would have otherwise gone to a hospital for such services. If an eligible ASC chooses to register as a hospital, the CMS will temporarily deregister it as an ASC during this time frame—meaning that it will receive payments according to hospital reimbursement rules rather than ASC reimbursement rules under the CMS fee schedules.5
This flexibility is available to any of the 5,732 ASC centers throughout the country and will immediately go into effect in 85 ASCs participating in the CMS’ Hospital Without Walls program.6 The extent to which this may impact WC changes is uncertain as regulatory adjustments and insurance carrier experience may be influenced.
CONCLUSION
The CMS has made substantial changes impacting the physician and facility fee schedules. The largest WC impacts are expected to come from 2021 CMS PFS revisions to RVUs for E/M services and the accompanying 3.3% decrease to the conversion factor. These changes will have varying impacts on individual states depending on their reliance on the CMS fee schedule.
The CMS also adjusted facility fee schedules. It will phase out the inpatient-only list over the next few years, which will increase flexibility and provide some patients with access to new procedures in an outpatient setting. The CMS will also temporarily allow ASCs to register as hospitals and perform hospital inpatient procedures to free up capacity at traditional hospitals that may become strained from the volume of services being provided to COVID-19 patients.
NCCI will continue to monitor these and other pertinent changes in Medicare reimbursement rules and how they may impact WC medical cost trends.
This article is provided solely as a reference tool to be used for informational purposes only. The information in this article shall not be construed or interpreted as providing legal or any other advice. Use of this article for any purpose other than as set forth herein is strictly prohibited.