INTRODUCTION
According to the Centers for Disease Control and Prevention, traumatic brain injuries (TBIs) are a significant cause of disability and death in the United States. A TBI is defined as a physical trauma to the head that alters the normal function of the brain.1 Those suffering from TBIs may not ever fully regain their social independence due to long-term side effects such as debilitating cognitive, mood, and behavioral problems.2 Based on the lasting effects of severe TBIs, these injuries have the potential to become disabling and very costly early on and over time.
- For active3 claims between Service Years 2013 and 2018,4 about 15% of permanent total claims with reporting through a second report had a TBI associated with the claim.5
- NCCI research on mega claims has found that brain and head injuries, such as TBIs, account for a significant portion of mega claims—17% of mega claims between $3 million and $5 million, and 30% of mega claims in excess of $10 million.6
- For active claims between 2013 and 2018, the average total incurred cost per TBI claim7 was more than double the average for all lost-time claims through a second report.
- As of 2018, lost-time TBI claims accounted for almost 5% of reported medical payments on all countrywide lost-time claims even though they represent only 2.5% of these claims.
This article will provide insight into the costs and medical services associated with TBI claims.
The statistics presented in this report are based on reported medical payments on claims from injured workers who are receiving lost-time benefits. No actuarial adjustments such as development or trend have been applied to the statistics.
BACKGROUND
TBIs are a common type of head injury in workers compensation (WC). In 2018, about 60% of head injury claims involved a TBI—up from 55% in 2013. The share of head injury medical payments associated with TBIs has also increased from 75% to 79% over this five-year period.
On average, TBI claims are costly. Through a second report, active TBI claims between 2013 and 2018 averaged about $136,000 in total incurred costs—an amount notably higher than that for all lost-time claims ($51,000). Approximately 2.5% of TBI claims exceed $1 million. These claims account for more than half of all TBI total incurred claim costs.
Among injured workers with active claims between 2013 and 2018, the largest share of TBI and lost-time claims originates from class codes in the goods and services industry group. However, with respect to medical payments, the contracting industry group accounts for the largest share of payments: 32% of total medical payments for TBIs and 18% for all lost-time claims.
Among all TBIs, the three most common causes of injury are (a) slips and falls, (b) being struck/injured by an object or person, and (c) motor vehicle accidents. More than 85% of medical costs from injured workers with a TBI can be linked to one of these three causes. Approximately one third of these payments are for services provided within the first week of the injury and two thirds within the first year, as shown below.
FACILITY AND PHYSICIAN SERVICES
Injured workers who have suffered a TBI typically receive an array of medical services. The chart below shows the share of payments by type of medical service for injured workers with a TBI. For comparison purposes, it also provides the share of payments for all lost-time claims. As shown, facility payments account for almost 50% of total TBI-related medical payments.
Hospital inpatient services account for the largest share of overall TBI-related facility payments. Due to the seriousness of TBIs, inpatient admissions can be expensive and lengthy. The longer length of stay (LOS) compared with all lost-time claims may be indicative of the need for monitoring oxygen levels, blood supply, and blood pressure as well as preventing further injury following a TBI.8
For 10% of stays, the LOS can be 30 days or more—much longer than the medians seen in the table below. These longer stays often reflect the severe consequences of a TBI, such as suffering from a coma and/or requiring mechanical ventilation for long periods of time. On average, costs associated with TBI claims are noticeably more expensive when surgical services are provided during the inpatient stay, which occurs in approximately 8% of stays.
The average paid-per-stay figures in the following table represent reported inpatient payments to date and, therefore, do not represent the full ultimate cost of these claims. Further, while claims may have multiple inpatient stays, the averages provided below are representative of a single stay, where a stay is defined as a hospital admission of a patient requiring hospitalization for at least one 24-hour period.
Hospital outpatient services also represent a significant portion of facility costs for TBIs. Computed tomography (CT) scans of the head or brain are the outpatient service that accounts for the largest proportion of payments made each year. These types of CT scans are frequently provided within the first week of injury to individuals suffering a TBI. CT scans of the cervical spine (i.e., neck) also account for a large proportion of hospital outpatient service payments and may indicate that injured workers who sustained a TBI have additional injuries beyond just the head.
Physician services account for the second largest share of total TBI-related medical payments. Due to the propensity of TBIs causing physical impairments, physical therapy consistently ranks as the top paid physician service. Injury evaluation and management, as well as occupational and cognitive therapies, are also common physician services.
DRUGS AND OTHER MEDICAL SERVICES
While physician and hospital costs account for a large share of medical payments throughout the life of a TBI claim, they represent a relatively smaller share of payments as the claim matures. After the first year, there is a significant shift in payments to drugs and other medical services,9 as shown in the graph below. The shift in medical payments to drugs after the first year of a TBI is relatively similar to that observed for all lost-time claim injuries. The shift in medical payments to other medical services after the first year of injury is much greater for TBIs—with about 28% of medical payments after the first year being for other medical services versus 7% for all lost-time claim injuries.
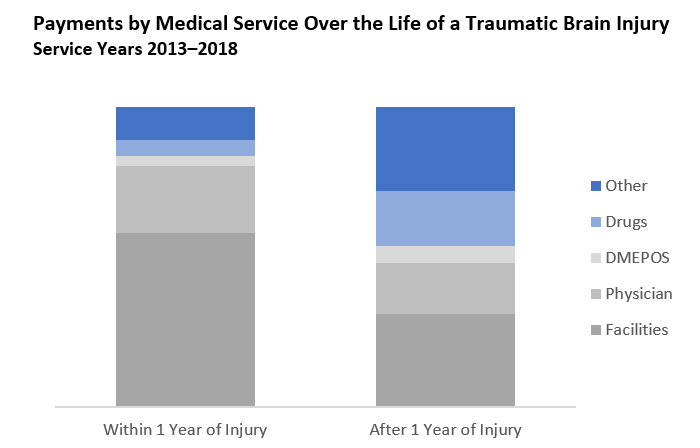
The shift in the medical payments as the claim matures may be indicative of the long-lasting effects of TBIs and the need for medical care that sometimes extends many years after the injury. While home healthcare services drive the largest portion of other medical payments, most drug costs can be tied to the prescribing of anticonvulsants and psychotherapeutics, which help treat the lasting effects of TBIs such as epilepsy and other cognitive disorders. Drugs not commonly thought of in the WC arena, such as Botox, have also started to appear. It has become one of the top 10 most paid TBI-related drugs as a potential treatment for muscle spasticity and post-traumatic headaches related to TBIs.10,11
CONCLUSION
TBIs may incur high costs early in the life of the claim and require medical care for many years after the injury. That care heavily comprises facility and physician-related services but may transition to home healthcare services and drugs as the claim matures. As mentioned before, many of these TBIs are the result of slips and falls, being struck/injured by an object or person, and motor vehicle accidents. Studies show that many TBIs and other head injuries are preventable when using personal protective equipment, securing items from falling, slip/fall prevention measures, and wearing a seatbelt.12 Ensuring that certain precautions are taken can be one effective method for preventing TBIs and their potentially devastating long-term effects.
This article is provided solely as a reference tool to be used for informational purposes only. The information in this article shall not be construed or interpreted as providing legal or any other advice. Use of this article for any purpose other than as set forth herein is strictly prohibited.