The Centers for Medicare and Medicaid Services (CMS) updates its reimbursement rules and rates for medical services each year. This report highlights the most relevant changes in the 2023 update and the potential impact on workers compensation (WC) medical costs.
Introduction
The National Council on Compensation Insurance (NCCI) monitors changes in CMS reimbursement rules and rates that impact WC medical costs. The impacts of these changes on WC medical costs vary by state. The medical service categories covered by medical fee schedules, the extent to which each fee schedule incorporates the CMS rules and rates, and the distribution of medical costs all influence how each state is impacted. NCCI’s report,
"Medicare Fee Schedules and Workers Compensation in 2022", highlighted noteworthy aspects of the 2022 update.
This report focuses on the 2023 changes to CMS fee schedule rates, the data CMS relied on to develop those rates, and other potentially impactful changes to the fee schedules for the following service categories:
- Facility
- Physician
- Durable Medical Equipment, Prosthetics, Orthotics, and Supplies
Facility Fee Schedule Changes
CMS Payment Rates and Data
Facility costs account for about 40% of countrywide1 WC medical expenditures. Many states base their WC facility fee schedules on the rules and rates CMS publishes to establish maximum allowable reimbursements (MARs) for procedures performed in a facility setting.
CMS publishes annual updates to its payment systems governing payment rates for services performed at the following facility types: hospital outpatient, ambulatory surgical centers (ASC), and hospital inpatient.
The table below displays the CMS payment system associated with each facility type:
For every facility type, CMS determines the payment rate for any given service by two main factors, the base rate and the relative weight.
CMS publishes a base rate and set of relative weights for each facility type. Within each facility type, CMS standardizes the base rate for all services while relative weights vary among services. Federal law requires CMS to update these factors annually.
CMS Base Rates
Each year, CMS updates base rates to account for changes in the prices of goods and services used by hospitals in treating Medicare patients. CMS refers to the update for changes in the prices of goods and services as the hospital market basket update. The 2023 market basket update was +4.1%. The chart below shows the final 2023 base rates across facility types. These 2023 base rates reflect the market basket update as well as other adjustments, such as adjustments for budget neutrality which vary by facility type.
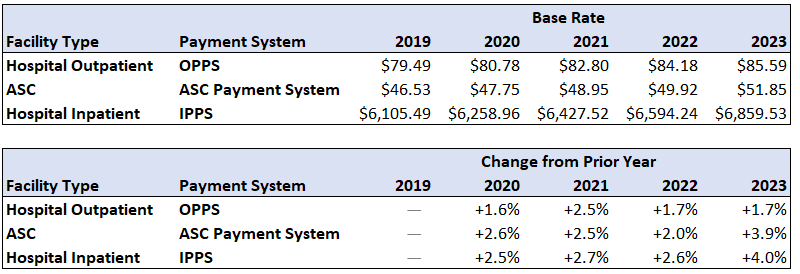
As seen above, CMS increased the ASC base rate from $49.92 in 2022 to $51.85 in 2023. This represents a +3.9% increase in the base rate for all ASC services in 2023. The +3.9% increase to CMS’s 2023 ASC base rate as well as the +4.0% increase to CMS’s IPPS base rate are greater than they have been over recent years and are close to the market basket update of +4.1%. On the other hand, the final change in the base rate for OPPS is notably lower than the market basket update but in-line with the 2022 change.
The change to the 2023 OPPS base rate is less than changes to other base rates because of a budget neutrality adjustment factor responding to the Supreme Court’s decision in
American Hospital Association v. Becerra.2 As part of section 340B of the Public Health Service Act, participating hospitals and other providers were allowed to purchase certain covered outpatient drugs from manufacturers at discounted prices. Starting in CY 2018, CMS paid a reduced rate for drugs and biologicals acquired through the 340B program. To achieve budget neutrality in anticipation of reduced drug prices, the CY 2018 OPPS base rate had a +3.19%3 increase. Following the Becerra decision, beginning in CY 2023, CMS will no longer pay reduced drug rates to 340B hospitals. This eliminates the drug savings introduced in 2018. As a result, CMS reduced the 2023 OPPS base rate by -3.09%,4 achieving budget neutrality and effectively reversing the increase introduced in 2018.
This -3.09% decrease combined with the +4.1% increase for the market basket update and other smaller annual adjustments resulted in the final +1.7% increase for the OPPS base rate.
CMS Relative Weights
CMS also updates the relative weights annually for each payment system.
This component of the rate setting process typically involves utilizing the most recent Calendar Year (CY) of claims data. In the 2022 update, CMS diverged from the usage of the most recent CY of claims data (CY 2020) in favor of CY 2019 data.5 In the 2023 update, CMS reverted to its use of the most recent available data (CY 2021) in rate setting.
Despite this difference in the data CMS used to determine relative weights, the 2023 relative weights did not significantly change within any of the facility payment systems.
The following sections highlight how these changes and others may impact facility costs in WC.
WC Hospital Outpatient and ASC
Hospital outpatient and ASC services combine to make up about two-thirds of countrywide facility costs in WC. Many states base both their WC hospital outpatient and ASC fee schedules on CMS’ OPPS.
The impact of the CMS base rate and relative weight changes on hospital outpatient and ASC costs in WC will vary by state depending on each state’s reliance on CMS in setting its fee schedule. There are many variations to how states incorporate the CMS factors. These varying methodologies can be generalized into three categories. These categories group states based on their reliance on the base rates and relative weights CMS publishes. Note that states without hospital outpatient fee schedules are not included below.
*These states also base their ASC fee schedules on Medicare’s OPPS.
When states update their Medicare-based or partially Medicare-based fee schedules, they incorporate the most recent CMS changes. Most of these states update their WC fee schedule annually, though some have less frequent updates.
The +1.7% increase to the CMS OPPS base rate will directly impact only states with Medicare-based fee schedules.
NCCI estimates the changes to the CMS OPPS relative weights may result in a small increase to outpatient and ASC costs in states with Medicare-based and partially Medicare-based fee schedules.
WC Hospital Inpatient
Payments for hospital inpatient services make up the remaining one-third of countrywide WC facility costs.
The impact of the CMS base rate and relative weight changes on hospital inpatient costs in WC will depend on the degree to which the state relies on CMS in setting its fee schedule. The following table categorizes states by their reliance on the base rates and relative weights CMS publishes. Note that states without hospital inpatient fee schedules are not included below.
The +4.0% increase to the CMS IPPS base rate will directly impact only states with Medicare-based fee schedules.
NCCI estimates the changes to the CMS IPPS relative weights may result in a small increase to inpatient costs in states with Medicare-based and partially Medicare-based fee schedules.
In addition to the increased base rates and revised relative weights, CMS published revisions to the following factors which may also impact WC hospital inpatient costs:
Low-Volume Adjustment
This adjustment provides for up to 25% in additional reimbursement for remote hospitals with low volumes of patient discharges. The additional reimbursement amount applies to the IPPS base rate, therefore impacting only Medicare-based states.
CMS initially introduced the low-volume adjustment in 2005. It subsequently expanded the criteria to qualify as a low-volume hospital and the formula to determine the percentage adjustment in 2011, and then again in 2018, providing additional benefits. These expanded benefits were set to expire on October 1, 2022, reverting the low-volume adjustment to the version initially implemented. However, Section 101 of the Further Continuing Appropriations and Extensions Act, 2023 extended the expanded benefits through December 23, 2022. Then, in late December of 2022, the Consolidated Appropriations Act of 2023 again extended the expanded benefits until September 30, 2024.
Fixed-Loss Outlier Threshold
CMS uses the outlier threshold to identify and determine additional reimbursement for inpatient episodes with costs that are significantly higher than usual. In 2023, CMS increased the outlier threshold from $30,988 to $38,788―a 25% increase. AK, CO, CT, DC, IN, MS, NC, SC, TX, and WV incorporate the CMS fixed-loss outlier threshold in its WC inpatient outlier provisions. This may mitigate the impact from the increase in the base rate in these states, as less claims will reach this threshold and qualify for higher reimbursement. The level of impact will depend on various factors, such as how each state incorporates the factor in its individual outlier provision as well as the prevalence of high-cost outlier episodes in each state.
Physician Fee Schedule Changes
Physician costs account for about 40% of countrywide WC medical expenditures. Like facility fee schedules, physician fee schedules in WC are often based on factors published in the annual CMS Physician Fee Schedule (PFS).
There are two general components involved in the calculation of the MAR for a given physician service: Relative Value Units (RVUs) and a conversion factor. RVUs are procedure-specific weights representing the relative expense to perform the procedure. The conversion factor is a constant factor applied to all non-anesthesia physician procedures that converts RVUs into dollars.
CMS publishes the conversion factor annually. CMS determines the conversion factor beginning with the prior year’s conversion factor and adjusts it with respect to multiple factors, including statutory requirements and compliance with budget neutrality.
The chart below shows the conversion factors for physician services for the latest three calendar years:
Statutory changes influence the 2023 conversion factor, including the expiration of the Protecting Medicare and American Farmers from Sequester Cuts Act that provided for a temporary 3% increase in physician payment rates. CMS initially published the physician conversion factor of 33.06, which would have been a –4.5% change from 2022. However, in late December, the Consolidated Appropriations Act, 2023 provided for a temporary 2.5% increase to physician services under Medicare. This resulted in the final 2023 conversion factor of 33.8872.
The second key piece of the physician MAR formula is the RVUs. CMS has not made significant changes to physician service RVUs since the 2021 update, which implemented large increases to evaluation and management codes. In the 2022 and 2023 CMS updates, RVUs have remained relatively stable. The 2023 update resulted in a moderate increase to RVUs across physician service categories.
The impact on WC medical costs will vary by state depending on the state’s reliance on CMS values in its rate setting. The interaction between the decrease in the conversion factor and increases in RVUs may result in a moderate decrease in physician costs for states which incorporate the CMS conversion factor.
Durable Medical Equipment, Prosthetics, Orthotics, and Supplies
The share of costs that Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) services represent varies by state, ranging between about 4% and 13% of WC medical costs.
CMS groups codes into two categories for the purpose of adjusting the DMEPOS fee schedule each year. The first group includes codes subject to the DMEPOS Competitive Bidding Program. The second group, comprising the majority of DMEPOS payments in WC, is for codes not subject to the Competitive Bidding Program. A CMS-calculated factor, composed of the Consumer Price Index for All Urban Consumers (CPI-U) and a productivity adjustment, updates the reimbursable amount for the latter group.
The table below shows the CMS-published fee schedule update factors for DMEPOS services for the four most recent calendar years:
As seen above, while the DMEPOS fee schedule for January 2022 increased the reimbursement for certain services by +5.1%―significantly higher than prior years―the January 2023 DMEPOS fee schedule increased reimbursement by +8.7%, even higher still.
The CPI-U from June 2021 to June 2022 of 9.1%, reduced by a 0.4% productivity adjustment, determined the 2023 update factor of 8.7%.
Concluding Remarks
CMS implemented higher increases to payment rates for facility services and DMEPOS in 2023 relative to recent years. Conversely, CMS decreased 2023 payment rates for physician services. The impacts of these changes on WC medical costs vary by state. The medical service categories covered by medical fee schedules, the extent to which each fee schedule incorporates the CMS rules and rates, and the distribution of medical costs all influence how each state is impacted.
Stay tuned for even more insights on medical costs that we’ll share during our Annual Insights Symposium. Presentations will be available on our website in mid-May.
This article is provided solely as a reference tool to be used for informational purposes only. The information in this article shall not be construed or interpreted as providing legal or any other advice. Use of this article for any purpose other than as set forth herein is strictly prohibited.
1Based on NCCI’s Medical Data Call. Includes data from the following jurisdictions: AK, AL, AR, AZ, CO, CT, DC, FL, GA, HI, IA, ID, IL, IN, KS, KY, LA, MD, ME, MO, MS, MT, NC, NE, NH, NM, NV, OK, OR, RI, SC, SD, TN, TX, UT, VA, VT, and WV. Unless stated otherwise, statistics are for Service Year 2021 WC data.
2www.supremecourt.gov/opinions/21pdf/20-1114_09m1.pdf.
3www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/Downloads/CMS-1678-FC-2018-OPPS-FR-Claims-Accounting.pdf.
4www.cms.gov/newsroom/fact-sheets/cy-2023-medicare-hospital-outpatient-prospective-payment-system-and-ambulatory-surgical-center-2.
5www.cms.gov/newsroom/fact-sheets/fiscal-year-fy-2022-medicare-hospital-inpatient-prospective-payment-system-ipps-and-long-term-care-0.