Social Security Disability Insurance (SSDI) is a federal program that provides benefits when a worker becomes disabled and cannot return to work. There is some obvious overlap with workers compensation (WC), which provides benefits when a worker becomes disabled in the course and scope of their employment. The National Academy of Social Insurance, using unpublished data from the Social Security Administration (SSA), reports that about 12% of SSDI recipients also collect, or have collected, workers compensation or public disability benefits.1 Based on other SSA-published data,2 NCCI estimates that about 88% to 92% of these dual recipients collect, or have collected, workers compensation. So, we estimate that about 10%, or a bit more, of SSDI recipients also collect, or have collected, workers compensation.
The relationship between the two programs is complex. In most states, SSDI benefits are secondary, and may be reduced, when WC benefits are being paid. However, in 14 states, known as reverse offset states,3 WC benefits, in some situations, are secondary, and SSDI benefits are not reduced.
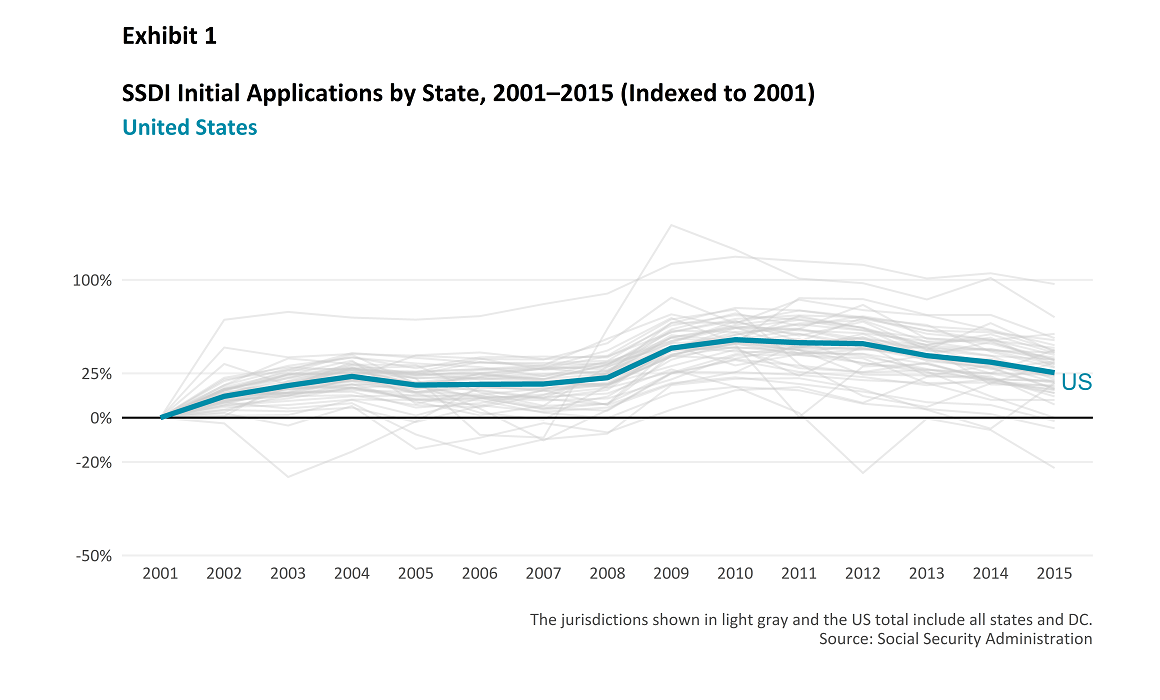
The number of SSDI applicants generally rose from 2001 to 2010; since 2010, the trend has reversed. Exhibit 1 shows SSDI growth in applications for the United States, indexed to 2001. We also show the application index for each state and the District of Columbia to provide context on how individual states vary around the US total. Some have suggested that the reason for the long-term increase in SSDI claims is that there has been a “race to the bottom” by state legislatures looking for immediate rate or loss cost reductions by lowering WC benefit levels, and that these lower benefit levels have caused an inappropriate cost shifting from WC to SSDI.
Cost shifting sometimes refers to a situation where one group underpays for a service, resulting in another group overpaying. In this context, cost shifting has a negative connotation. However, sometimes programs change to bring outcomes more in line with intent. If changes to a system bring its outcomes closer to intent, that should not be viewed as negative. Let us more closely examine WC benefit-level changes over this period, and possible impacts on cost shifting between WC and SSDI.
How Much Have Benefits Changed?
Benefits will go up over time due to wage inflation. Additionally, annual changes in minimum and maximum weekly benefits in many states are automatically implemented to keep up with inflation.
When WC legislative benefit changes can be reasonably quantified at the time of enactment, NCCI will do so and recommend rate or loss cost-level changes based on that analysis. The next two exhibits focus on quantified benefit changes other than the impact of inflation (on both wages and the minimum/maximum weekly benefits).
Exhibit 2 shows the cumulative impact of these quantified benefit changes from 2000 to 2015 for Permanent Partial Disability (PPD) indemnity benefits, and Exhibit 3 does the same for Permanent Total Disability (PTD) indemnity benefits. Although five states have significantly reduced PPD indemnity benefits, the vast majority have either increased these benefits or held them constant. Only two states have significantly reduced PTD indemnity benefits. We will examine a few of these benefit reductions later in this paper, but overall it’s clear that there has been no “race to the bottom.”
Workers Compensation, Medicare, and Cost Shifting
As discussed above, cost shifting, in and of itself, is not necessarily bad—sometimes it is the result of realigning practices with the original intent of a program. For example, SSDI beneficiaries receive Medicare to cover their medical expenses (after a waiting period). Medicare is not supposed to pay for medical costs due to covered work-related injuries; that is the responsibility of the WC insurer or other WC payor. This was established by the 1965 Medicare amendment to the Social Security Act.
To help ensure compliance, the Centers for Medicare & Medicaid Services (CMS) has a process for reviewing proposed Medicare Set-Asides (MSAs), which are the parts of WC settlements that cover costs that Medicare would otherwise pay.
Strengthening enforcement of Medicare’s secondary payer role from 2001 to the present has had a large cost-shifting impact. Claims subject to MSAs are often quite large. In NCCI’s 2014 study on MSAs,4 we found that insurers had to increase that component of their overall settlement on these claims in 2010 by roughly 60%, which is approximately $40,000 more per claim subject to an MSA. Once this became a more established practice, the average difference between the proposed and approved MSAs was much smaller (16% in 2015).
This was a major cost shift to WC from Medicare (which also covers SSDI beneficiaries). However, to the extent that the increases were appropriate to protect Medicare’s interests, this cost shifting is appropriate.
Has There Been Cost Shifting Between WC and SSDI?
Given the offsets that exist, there will inherently be some cost shifting between WC and SSDI for dual beneficiaries. When WC raises benefits for permanent disability, all else being equal, SSDI payments to dual beneficiaries will decrease in those states that do not have reverse offsets for the relevant benefit type; further, in these states, when WC lowers benefits for permanent disability, then SSDI expenditures increase, all else being equal.
WC compensability requirements are sometimes tightened to ensure that injuries resulting from nonwork-related factors are not compensated under the WC system. When this happens, there may be some cost shifting to SSDI. As with the MSA example, this just brings things back to the way they were intended.
Some Specific State Reforms
We talked about dual beneficiaries, but what about WC claimants who aren’t currently SSDI beneficiaries? Would a cut in benefits, or a tightening of state WC compensability standards, induce injured workers to file for SSDI when previously they would not have? Let’s look at some specific instances.
Florida
Florida’s SB 50A, enacted in 2003, was estimated to reduce PPD benefits by almost 20% and even more for PTD. The focus of the reform was not just the level of benefits, but also to reestablish some objectivity for qualifying for PTD.
For most WC benefit types, Florida is a reverse offset state in that the WC benefits for dual recipients may be reduced. However, if the Florida WC benefits are PPD, then the SSDI benefits may be reduced as they would be in a standard offset state. This benefit change decreased the WC offset resulting in SSDI expenditures increasing for dual beneficiaries. However, the nature of the change in PTD was predominantly around compensability requirements. To the extent that the law eliminated PTD awards that weren’t for permanent and total disability, it just brings the WC benefits in line with the original law’s intent.
What happened to new SSDI applications? Exhibit 4 highlights the Florida SSDI application index from 2001 to 2015. After remaining flat in 2004, SSDI applications decreased in 2005 and again in 2006. Applications increased in 2007 and started to really climb in 2008.
There may be some individuals who were motivated to file SSDI because of the reform (especially if they were no longer eligible for PTD benefits under the WC Act), but the benefit reduction in 2004 does not explain the magnitude of the increase in SSDI applications a few years later. While there may have been some delayed impacts of the reform, the recession is the more probable cause of the increase in applications.
This assessment is supported by comparing the Florida application index to countrywide. The Florida pattern looks similar to that of the country, with 2004 being the prerecession high point for applications, followed by significant increases during the recession (which hit Florida harder than most states).
Oklahoma
Oklahoma has had multiple significant changes in PPD benefits since 2000. The most recent one was SB 1062, effective February 1, 2014. This bill decreased the maximum duration for nonscheduled PPD indemnity benefits by 30%, and changed the version of the
AMA Guides used to determine the degree of disability from the 5th edition to the 6th edition, which is generally expected to produce lower average estimates of permanent impairment. Therefore, one area of cost shifting will come from the reduced offset on dual beneficiaries (which we will quantify in our upcoming paper). But what about new SSDI applications?
Exhibit 5 shows that after both the 2005 and 2014 law changes, applications decreased—in contrast to the increase observed beginning in 2009. Once again, the overall level of SSDI applications seems more impacted by the recession than the benefit change.
Montana
Montana HB 334, enacted in 2011, made several changes to WC benefits; one of the more notable is that medical services after 60 months from the date of injury require special authorization. Is there evidence that the fear of not having all of one’s medical expenses covered for a WC injury leads to more applications? Once again, we see a familiar pattern in Exhibit 6—a surge in applications during the recession but no increase in applications after the benefit change.
Other Interactions Between WC and SSDI
Some have asserted that an increase in denials of injured worker claims in WC is responsible for SSDI’s increase in applications. NCCI does not have data on WC denial rates, but one wonders—if changing denial rates is the reason SSDI applications increased from 2001 to 2010, is it also the reason SSDI applications have been declining since 2010? The economy’s stumble and recovery seem a more likely cause.
Summary
There may have been some cost shifting from WC to SSDI in the handful of states that have reduced benefits—but the idea of a “race to the bottom” is not borne out by the facts.
In many states, much of the cost shifting in recent history has been in favor of SSDI due to WC benefit increases (or in favor of Medicare, due to strengthening enforcement of Medicare’s role as a secondary payer).
Cost shifting is not necessarily bad in and of itself. It may just bring things back in line with the original intent of a program—whether that program is WC, SSDI, or Medicare.
What’s Next?
As mentioned earlier, the complexity of the WC/SSDI interactions will be explored in depth in a paper to be released later this year. NCCI is continuing its research activities to be fully prepared to assess any significant changes in the WC/SSDI relationship.
Acknowledgments
We thank Matt Schutz and Bruce Spidell for valuable contributions to this article.
This article is provided solely as a reference tool to be used for informational purposes only. The information in this article shall not be construed or interpreted as providing legal or any other advice. Use of this article for any purpose other than as set forth herein is strictly prohibited.